

The Science to immediately END Half of All Vaccines used on Earth.

The LEE String Theory that is more Fact than Theory, Again CLOTS
What was the point of the booster COVID mRNA vaccine given within two months of the first vaccine? Wasn’t the goal to increase the amount of COVID neutralizing antibodies? It’s hard to imagine another goal than that, but please correct me if I am mistaken. Let’s assume that was their goal in administering a second COVID mRNA vaccine with a few months of the first vaccine, the “booster” vaccine. Let me explain how the “booster” vaccine given within a few months of the first vaccine actually drastically decreased the amount of COVID antibody in the blood for at least a few weeks and simultaneously dramatically increased the risk of CLOTS and tissue damage downstream from the CLOTS.
Here is the bizarre twist. As I described in the previous section, having free spike antigen (as opposed to the antigen being attached to a virus particle) allows formation of antibodies to both the top of the spike antigen and the bottom of the spike antigen, at the absolute minimum. When a COVID virus presents the spike antigen to B-lymphocytes, only the TOP of the spike antigen is presented for later antibody production. But, for a free spike antigen not attached to a virus particle, all sides of the spike antigen molecule can produce corresponding antibodies. It is impossible for a vaccine scientist to argue this point and say otherwise.
Following the first COVID mRNA vaccination, a patient formed COVID antibodies to both the TOP and the BOTTOM of the COVID free spike antigen. Many more distinct antibodies may have formed, but we only need these two and the spike antigen to produce strings.
Following the second COVID mRNA vaccine, we are absolutely certain of three facts.
1) COVID antibodies to the top of the spike antigen are present.
2) COVID antibodies to the bottom of the spike antigen are present.
3) Free spike antigen is present. What a tangled web (of antibodies) we weave once we begin to deceive (the liar that pretended he was a good scientist for 38 years, fauci).
It cannot be refuted. Following a booster COVID mRNA vaccine given within a few months of the first COVID mRNA vaccine, there will be present in the blood at the same time COVID antibodies to the top of the spike antigen, COVID antibodies to the bottom of the spike antigen, and spike antigen. No vaccine scientist on earth can dispute these three points.
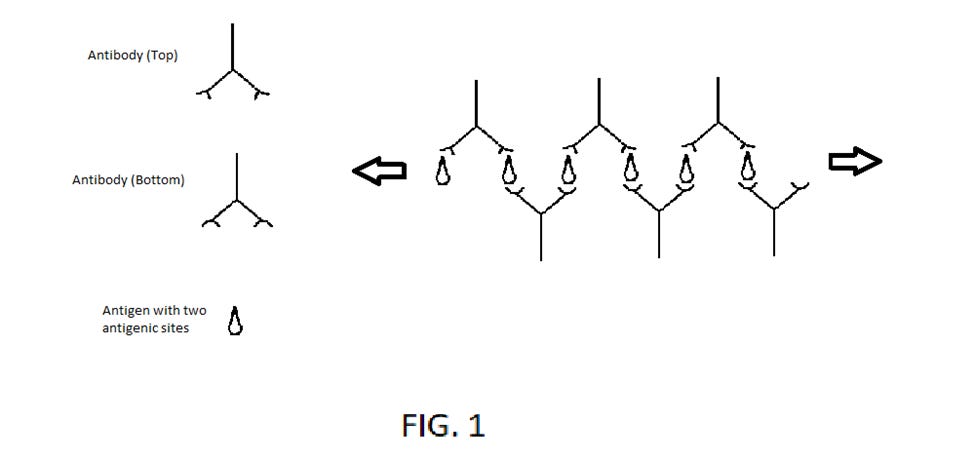
Referring to FIG. 1, the booster vaccine results in the body producing spike antigen that is now present in the blood/lymph. One arm of an IgG (Top) binds to the top of the spike antigen (1). One arm of an IgG (Bottom) binds to the bottom of the same spike antigen (1). The second arm of an IgG (Bottom) binds to another spike antigen (2). One arm of a second IgG (Top) binds to the same spike antigen (2). The second arm of the second IgG (Top) binds to a third spike antigen (3). And the pattern can continue indefinitely, producing thick strands of antibody/antigen complexes. There can be many separate “strings” of alternating IgG (Top) and IgG (Bottom) antibodies. Can you see how this meshwork of strings is the basis for long gelatinous, clots?
There can be infinite variations of the resulting meshwork patterns and size that can emerge from strings of antibodies formed from the mix of IgG antibodies and IgM antibodies and the spike antigen that act as glue connecting 1) antibodies both IgG and IgM to the top of the spike antigen and 2) antibodies both IgG and IgM to the bottom/side of the spike antigen. The strands of antibodies can be of variable length and some strands may form into balls not that different from balls of string. It is not inconceivable that some of these “balls” of antibodies grow large enough to block blood vessels, with all the downstream damage from blocked blood flow.
Lattice structures formed from immune complexes (antibodies binding to their respective antigen) are a well-known phenomenon and have been extensively studied. Lattice structure formation is affected by many factors. With the COVID spike antigen, we have an extremely unusual situation that dramatically increases the size and length of these structures. With a natural COVID viral infection, antibodies are only formed to the top of the spike antigen. However, free spike antigen generated following the COVID mRNA vaccine results in the production of at least two distinct antibodies, to the top and bottom of the spike antigen. This creates a bizarre situation following administration of the booster COVID mRNA vaccine. There are antibodies now present to the top of the spike antigen and to the bottom (or stalk portion) of the spike antigen.
This opens the possibility for a never-ending weave of lattice structures or strings, until the respective antibodies and spike antigen becomes unavailable due to the formation of extensive lattice structures (and strings of variable length) which create extended clots. The chances of a COVID antibody molecule formed in response to the first COVID vaccine binding a natural COVID virus is at least a million times less than the chances of that same COVID antibody molecule combining with a spike antigen and being found within a meshwork of antibodies. That is why I call this the “Lee string theory that is more fact than theory.” This is why the resulting meshwork of antibodies is the “MAIN EFFECT” of the booster COVID mRNA vaccine. If a side effect of the COVID mRNA vaccine occurred as infrequently as the chance of their COVID antibody binding a COVID virus in the lung, the vaccine scientists would not even list it as a “side effect.” Again, this is exactly why I state that this string formation of antibodies IS THE MAIN EFFECT of the COVID mRNA vaccine.
It is well known that immune complex clearance is affected by the size of the lattice structure. Because of the unusual situation with the free spike antigen resulting in production of at least two different antibodies, immune complexes can criss-cross and form alternating connections with other immune complexes, in ways that would be extremely unlikely if only antibodies to the top of the spike antigen are present. The larger the meshwork of antibodies with spike antigen as the glue connecting the various antibodies, the more unlikely that the normal clearance mechanism can be effective.
Suppose a patient is deficient in certain complement factors. In that case, the normal process of removing “immune complexes” from the blood is markedly diminished, and the build-up of pathologic immune complexes will lead to glomerulonephritis and vasculitis throughout the body. Since the booster COVID mRNA vaccine produces “immune complexes,” giving the booster without knowing whether a patient has adequate complement factors will put the patient at a significantly higher risk for tissue damage, especially given the extended meshwork of antibodies that will inevitably form. Giving the COVID booster mRNA vaccine to a patient with deficient complement factors can result in a build-up of pathologic immune complexes, which can further cause glomerulonephritis (including the risk of kidney failure) and vasculitis. The presence of vasculitis in the coronary vessels can lead to heart attacks.
Similar to how pine needles and leaves can clog gutters and prevent water flow, strings of antibodies, platelets, white blood cells, red blood cells, and coagulation activation can create blockage of blood vessels all over the body. All you have to do is imagine how your shower drain can be blocked by strands of hair and gunk.
Every vaccine that provides an antigen with more than one antigenic site (almost every vaccine) creates this identical situation when a booster is given within a few months of the first vaccine (if the antigen is small enough so that each arm of the antibody can bind to separate antigen molecules). All booster vaccines using antigens fitting this size criteria should be immediately stopped worldwide until this is completely vetted.
There will be many more important medical discoveries from this hypothesis but in the interests of quickly preventing more patient suffering/death, I am releasing this information now.
I'm back on twitter with a second account, who knows for how long. lasikeyecenter1 is my handle. an old account I never used.
You've been missed on twitter, Dr. Lee !! Hope you're well 💌